
Debating Ideas is a new section that aims to reflect the values and editorial ethos of the African Arguments book series, publishing engaged, often radical, scholarship, original and activist writing from within the African continent and beyond. It will offer debates and engagements, contexts and controversies, and reviews and responses flowing from the African Arguments books.

Africa may be on the cusp of a third wave of Covid-19. A WHO briefing dated 20 June suggests the disease is “resurgent” in Algeria, DRC, Liberia and Sierra Leone, and places Benin, Gambia, Guinea, Mali and Senegal on an “alert” list.[i] A report in the Financial Times (23 June) argues a third wave has already started, citing major problems in southern Africa and Uganda (where the president has reported that hospitals are “full”).[ii]
Assessing the situation still runs into problems of lack of community testing or genomic sequencing. But is there a more general problem with our basic mental modelling of the disease? Does thinking in terms of waves distort our sense of what we need to do?
Waves would be helpful if we could, for example, see a row of countries falling to Covid-19 like dominoes, say in a line across West Africa from Nigeria to Senegal. Analysts have also considered temporal linearities, by suggesting that countries with experience of Ebola may have been better able to protect against Covid-19. Evidence, however, is lacking. Nothing seems to stand up. Covid-19 has reached everywhere in Africa, but in no apparent order.
The dubiousness of wave thinking is at last underlined by the fact that the worst Ebola-affected countries – DRC, Liberia, and Sierra Leone – are now on the latest WHO resurgence list for Covid-19. If prior experience of Ebola did once help resist Covid-19 the effect has ended.
Ebola did have one clear lesson to teach Covid-19, however, that those attempting to conceptualise the epidemic needed to think locally. Yes, Ebola in West Africa in 2014 did spread from the Guinean interior to the coastal cities, but closer analysis suggests that the pattern was saltatory (jumpy). The disease hopped rapidly from the rural interior to the cities, and then back into the interior, in no apparent order, with some localities being totally by-passed for infection, and others experiencing intense outbreaks. This focused attention on knowing in detail what exactly happened, locally.
In 2014 rural Sierra Leone was divided into 149 administrative chiefdoms. The national records of laboratory-confirmed Ebola cases show that as many as 60 percent of cases were confined to just 14 chiefdoms, and that 39 chiefdoms had no cases whatsoever. Not all these chiefdoms without cases were in isolated locations either. Some were surrounded by a large number of active cases in neighbouring chiefdoms.
Numerical analysis looked for linear patterns and failed to find them. Researchers concluded that the West African Ebola epidemic was characterised by “heterogeneity” – a fancy word suggesting a myriad of local factors (Garske et al. 2016, Krauer et al. 2016). On further enquiry it appears that good or bad luck often played a major part. Outbreaks, in short, required to be analysed in fine-grained detail, case by case. No general story of Ebola infection is there to be told.
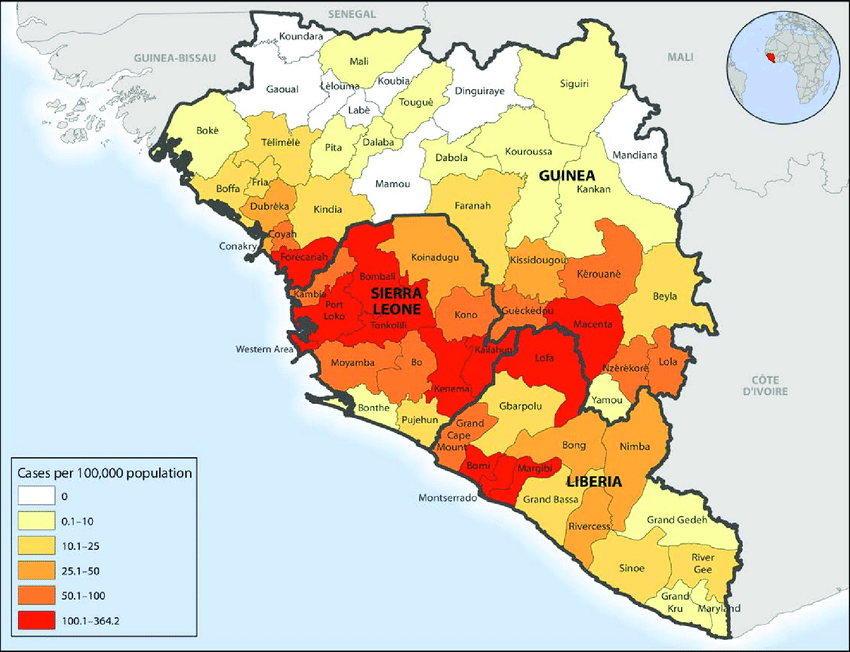
Tracing Ebola infection sequence in Sierra Leone
Maybe we now need to take this lesson and apply it to Covid-19 in Africa? With Ebola, stringent attempts to exclude infection worked for a time, up until the point some strong-minded or desperate individuals or group broke the rules, and then an outbreak would occur, driven by the inescapable mathematical logic of exponential growth. Maybe with Covid-19 we also need to see it in terms of localities, and local agency, and not in terms of generalities at all? Maybe, in fact, we need to bring the story of infection closer to home?
The Ebola situation was governed by a lack of appreciation of why some families might feel impelled to break the rules. Their intention was almost certainly not to be defiant, but rather due to a lack of awareness of the consequences. This included lack of preparation by the authorities to cope with obvious needs, such as practical provision for quarantine and social distancing. People cannot stay at home, and apply social distancing, unless someone provides food, water and wood for cooking.
Fighting infection then became less like building bunds against a spreading flood, and more like dealing with the likelihood of many fire outbreaks on tinder-dry grassy ground, where no sooner is one flare-up addressed than fire-fighting teams have to rush to another. There is no particular pattern. What counts is having enough teams and resources to deal with outbreaks quickly, before they get out of hand. It would certainly help if householders were among those first jumping up to stamp out the fires.
The solution for Covid-19 in Africa can now be envisaged in these fire-fighting terms. Vaccines will provide a foundation for ending the pandemic but are not a complete response.[iii] Other family-level interventions to reduce transmission are also needed. Masks, ventilation and social distancing are the immediate tools.
People can deploy these tools for themselves, but will they? The answer seems to be only if local agency is fully engaged. Only part of the problem of application is supply logistics. An equally important part is the failure of authorities to appreciate the need to engage people over the social logic of preventing an air-borne disease in the family as much as in the public domain.
With masks and faces the ritual and performative dimensions are as important as having the mask. A better understanding by responders is needed, in specific cultural contexts, of how people see masks, and interpret their use. What Erving Goffman once called the “the presentation of the self in everyday life” would be a useful lens. Epidemic control is largely a matter of how we (the potentially infective agents) see ourselves moving within our daily community settings, and assuming responsibility for others, starting with our responsibilities at home. Goffman (1959) should be on the reading list of all Covid-19 responders, where a degree in household studies, or fashion, might be as useful as a degree in epidemiology!

Credit: The Lancet
Sufficient numbers of people will eventually be vaccinated to provide what some epidemiologists term “herd immunity”. But this is a catastrophically bad term, and should immediately be replaced with something human, like “collective immunity”. Herds only become immune through mass infection and potential high death rates. Humans can increase their immunity by paying attention to their responsibilities to the group (by accepting vaccination and keeping to rules on masks and social distancing).
On vaccine hesitancy
The “go local” message also needs to be applied to vaccination. Vaccinators need to be prepared to listen to neighbourhood voices before they begin their work. People have many reasons to be cautious about vaccination. Some are based on bitter experience of vaccines going wrong (polio in Africa is an example). Others are based on emotional reaction – often forged by feedback in groups. All these reasons require to be thoroughly well understood, and none should be dismissed out-of-hand as the rantings of the ignorant.
We have spent time listening to and documenting some of these objections in Sierra Leone. It is striking how often they are expressed in group or family terms.[iv] For example, “I will wait until I see how my companions react.” “Vaccines have been designed by Westerners to reduce the number of my African brothers and sisters in the world.” But equally, people seem to respond more positively to vaccine advocacy that stresses collective concerns. “This vaccine prevents you from passing on sickness to others you care about.” “We will take the vaccine to ensure that we Africans are not wiped out by the disease.”
One of us (EYM) even tried the experiment of talking in terms of the virus’s own need to survive, arguing with a hesitator that vaccination helped disease agent and host to reach a compromise. This meant in turn that vaccination would not completely eliminate the possibility a human agent might still spread the disease, so the vaccinated person had to continue to think about protecting others. Talk of accommodation and co-existence (as applicable to malaria as to Covid-19) seemed surprisingly persuasive in turning doubts to acceptance. As humans we seem wired to respond positively to cooperation and compromise. Difficult truths are often more palatable than politicians appear to suppose.

Co-author on a testimonial collection field trip
A positive response of a few then begins to translate into a more general shift in perception that indeed vaccination is part of the answer to a collective challenge, especially when tied to other behaviours signalling community support, such as wearing a mask as an expression of social responsibility and group solidarity.
So probably it is now time to drop talk of “waves of infection” and “herd immunity”, and instead to embrace a language of human collectivity. “We do this because we care about our community and its survival.” This way epidemiology is reclaimed from the experts – words like “heterogeneities” sound grand but explain little – and is returned to the people where it belongs. Infection control begins at home.

The author’s book on Ebola in West Africa was published in the African Arguments series
Endnotes
[i] WHO Health emergency and risk assessment, Covid-19 pandemic in West and Central Africa, update as of 20 June 2021.
[ii] ‘Africa’s third wave: “What haunts me a lot is the Indian scenario”’, Financial Times, 23 June 2021, https://www.ft.com/content/76c37996-490d-42da-9568-44e689b4b662.
[iii] See Zamia Stamataki, ‘Vaccines are not magic bullets – we’ll still have to take precautions’, The Guardian, 22 June 2021, https://www.theguardian.com/commentisfree/2021/jun/22/viruses-wearing-mask-england-vaccines
[iv] This point about community responsibilities has also been strongly emphasised by a group of behavioural scientists advising the British government on pandemic response (Bonell et al. 2020).
References
Bonell, C. et al., 2020, ‘Harnessing behavioural science in public health campaigns to maintain “social distancing” in response to the COVID-19 pandemic: key principles’, Journal of Epidemiology and Community Health 74 (8).
Garske, T. et al., 2016, ‘Heterogeneities in the case fatality ratio in the West African Ebola outbreak 2013–2016’, Philosophical Transactions of the Royal Society of Biological SciencesB. Biological Sciences 2016, 372.20160308. Doi.org/10.1098/rstb.2016.0308.
Goffman, E., 1959, The Presentation of Self in Everyday Life. Edinburgh: University of Edinburgh Press.
Krauer, F., et al, 2016, ‘Heterogeneity in district-level transmission of Ebola Virus Disease during the 2013–2015 epidemic in West Africa’, PLoS Neglected Tropical Diseases10 (7): doi.org/10.1371/journal.pntd.0004867.
Richards, P., et al., 2020, ‘Re-analysing Ebola spread in Sierra Leone: the importance of local social dynamics’, PloS One, doi.org/10.1371/journal.pone.0234823.

