Debating Ideas is a new section that aims to reflect the values and editorial ethos of the African Arguments book series, publishing engaged, often radical, scholarship, original and activist writing from within the African continent and beyond. It will offer debates and engagements, contexts and controversies, and reviews and responses flowing from the African Arguments books.

Source: Quartz Africa
We live in a world of nations, and Covid-19 (the disease caused by the SARS Cov-2 virus, first emergent in China in late 2019) has been addressed nationally. Nationalism under a pandemic is a recipe for trouble. Having bungled its Covid-19 response to the point where it has one of the worst death rates in the world the flag-waving British government daily pumps out information about how rapidly it has rolled out vaccination to its vulnerable citizens. Of potentially greater significance, however, was the news in the last week of February 2021 concerning the arrival in Ghana of the first consignment of vaccines for Covid-19. This was welcome evidence of a global response to a global threat.
The Ghana vaccine delivery was an initial event in an internationally coordinated Covax programme to provide Covid-19 vaccines across all countries. The world is dealing not with an epidemic but with a pandemic. Pandemics know no borders. If the disease is not controlled everywhere it is controlled nowhere. This is why we need to talk more about global impacts and global responses. The WHO provided a significant focal point for these conversations when it made available the graphic reproduced below. This shows the trajectory of the disease across all regions of the globe from the beginning of the pandemic. In it, we see a surprising pattern – that the pandemic of Covid-19 appears to move in step across all global regions. In particular, a recent downturn in Europe and North America appears to be matched in other regions of the world.
The pattern for Africa is especially interesting. In the WHO graphic (look closely at the bottom of the diagram) the continent shows two modest peaks of infection – one centred around mid-2020 and the other around Christmas and New Year 2020–21. The second of these waves is currently in a downward phase, in apparent coordination with recently tumbling rates of infection in Europe, and more especially in the Americas. This is not time for complacency. Even now global figures may already be on an upturn. But the point is that we need to better understand these variations.
There are two distinct features of the global pattern revealed in the WHO graphic. One is the large difference in infection rates across different regions. But equally striking is the element of global co-variation. Put simply, why do waves of infection in Africa track those in Europe and the Americas when the infection levels are so different? Is there a mechanism of coordination, and what does that imply for methods of control?
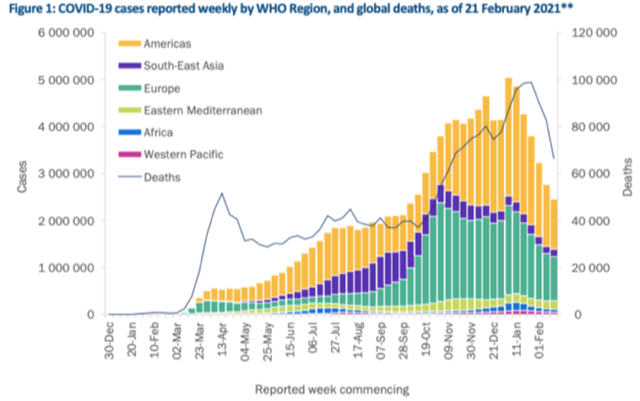
Reported Covid numbers by region and globally. Source: WHO
Initially, commentators assumed that if the disease was bad in Europe and North America it would be worse in Africa, but this has turned out to be far from the case. Africa continues to have a low level of cases. The reasons for the low overall level of cases in Africa still remain to be decided by research. But key factors seem to be a youth-oriented age profile (the disease affects the young much less seriously) and higher levels of daily interaction taking place out of doors or in well-ventilated places. Work that might be expected to take place in factories or warehouses in Europe or North America is often undertaken in the open air or in open-sided sheds in Africa. Socialization takes place on verandas or under shade rather than indoors. An over-crowded bus is probably much less infectious when all the windows are wide open, as they will be when the vehicle is elderly and operating in a tropical climate.
It took some time for health advisors to wake up to the role of ventilation in spread of Covid-19. Recently, however, the language of prevention has begun to change. It is now considered unlikely that crowded beaches cause infection. Children are deemed to be at little risk playing together in the open air. The new mantra is “ventilate, ventilate, ventilate”.
But now we turn to the surges within Africa, despite low overall numbers. How can these be explained?
Some consider that climate plays a part. South Africa has among the highest rates of infection in Africa – over 1.5 million cases, making it comparable (per capita) with many European countries, though case numbers from the second wave, as elsewhere in the continent are currently easing. It has a sub-tropical cold season. Climate cannot be the only factor, however. After controlling for population size, Nigeria has an infection rate 1.5 times higher than Sierra Leone (a country with a similar hot and humid climate). In this second case perhaps we have to factor in the better built environment in the oil-rich country? Air-conditioning might make the humidity more bearable, but it may also be circulating the virus.
The very low rates of spread in Sierra Leone tell us a bit more about pandemic mechanics. The country was badly affected by the 2014–15 Ebola epidemic. Both government and the people reacted to Covid-19 as if it was Ebola (that is, they responded rapidly, and hard). Well-tried case-finding and isolation methods were immediately applied, slowing the rate of infection spread. Quarantine was in a military hospital and patients were well cared for.
Nevertheless, the country experienced two surges in keeping with the Africa-wide pattern revealed in the WHO graph. The recent second wave of infection appears to have been boosted by Christmas holiday season travel, especially from UK and the USA. Not all visitors appear to have followed the rules on self-quarantine. Some contact addresses were incorrect and perhaps not all PCR test certificates were genuine (fake certificates are reportedly for sale online). The government was forced urgently to reinforce its travel regulations.
This case may give us an insight into one of the possible factors underpinning pandemic coordination. If “leaky” travel regulations foster surges of infection, then a general level of decline in the most severely affected countries will also translate into decline of infection in other regions as well. This would be important to establish, since it implies that infection control in the worst affected countries will have a disproportionately beneficial impact on infection levels overall. It is known that many individuals contribute little or nothing to spread of Covid-19 but a smaller number of infected people are responsible for a large number of infections. In effect, it may be the case that this applies at the international level also. Surges and recessions in Africa respond to surges and recessions of the disease in other parts of the world.
If this is the case, it is a reminder of an important fact – that we are dealing with a pandemic, not an epidemic. Responders need to think internationally, not nationally. Countries like Britain could take justified national pride in the speed of their vaccine roll-out if it was more clearly understood that energetic reduction of infection levels in the worst affected countries benefits the whole world. This would be an instance of confronting a pandemic with pandemic-scale political thinking. This is needed because a major destabilizing threat to pandemic control is the existence of a global pool of mutations, fostered in countries which came closest to losing control of the disease (currently Britain, South Africa and Brazil, but other mutations are already in the mix, for example from New York and California in the United States).
One case for which we urgently need to apply this newly-fostered pandemic-scale of thinking is to the question of whether or not the Tokyo Olympic Games should proceed, since this is a global event seemingly potentially perfectly aligned to mix and spread more effectively the common pool of Covid-19 variants. Participants and spectators will need to do more to guard against the danger of super-spreading of viral mutations than to have a valid PCR test certificate and contact address. They will also need to have trained their minds thoroughly in understanding how the virus moves.
Ought we to go further?
Now we have all woken up to the true meaning of the word “pandemic” how sensible is it to plan to bring back potentially bioactive materials from Mars? Closer to home, how sensible is it to have gain-of-function and dual-use research in so many laboratories with such unfortunate records of biosafety breakdown?
How we debate these global issues is of crucial importance. They cannot be left to governments, since we have seen all too clearly in the pandemic that governments react to the closest threat at hand. This implies the need for a global citizen-based conversation about pandemic preparedness. Covid-19 has suggested that citizens sometimes see further than their own governments, and the raising of their strategic voices should be encouraged. Africa has always been open to the world, and now has an important part to play in the debate about the true meaning of the word “pandemic”. Sport is fine as spectacle but perhaps what we really need at this moment is an Olympics of citizen debate?